IMPORTANT FACTS REGARDING COVID-19 AND ITS MANAGEMENT
Foreword
Purpose of this Webpage. This webpage is designed to provide certain facts about COVID-19, such as its fatality rate and how it might be, in the majority of cases, effectively and quickly cured. I initially created this site in order to placate fears people might have regarding COVID-19 and its variants as a consequence of deliberate exaggeration of its lethality by the media and Public Health Authorities around the world.
Submission to the Senate Enquiry on Excess Deaths in Australia. The political world is now slowly awakening to the fact there has been perpetrated a huge fraud and that, as a consequence of this and the foolish over-reaction of authorities, many people needlessly lost their lives for want of effective early treatment whilst many millions more are either dead or seriously injured as a consequence of being encouraged or coerced (through the threat of their employment being terminated) to submit to a series of anti-COVID-19 Injections (ACIs) based on mRNA technology. Doctors who spoke out against this have been deregistered and held in limbo without their cases being expeditiously heard. This "slow-walking" of the process, preventing doctors from earning a living, seems to be deliberate. It is intended to hurt the doctor financially and emotionally and to deter any other doctor from voicing their concerns or expressing a critical opinion on this matter. On 17 May 2024, I forwarded a submission to the Senate Enquiry on Excess Deaths in Australia. This submission will give the reader some insight into what transpired. That submission may be found here, "Excess Deaths In Australia - Senate Inquiry", with its supporting annexes.
Please share this with all of your contacts. It may save a life.
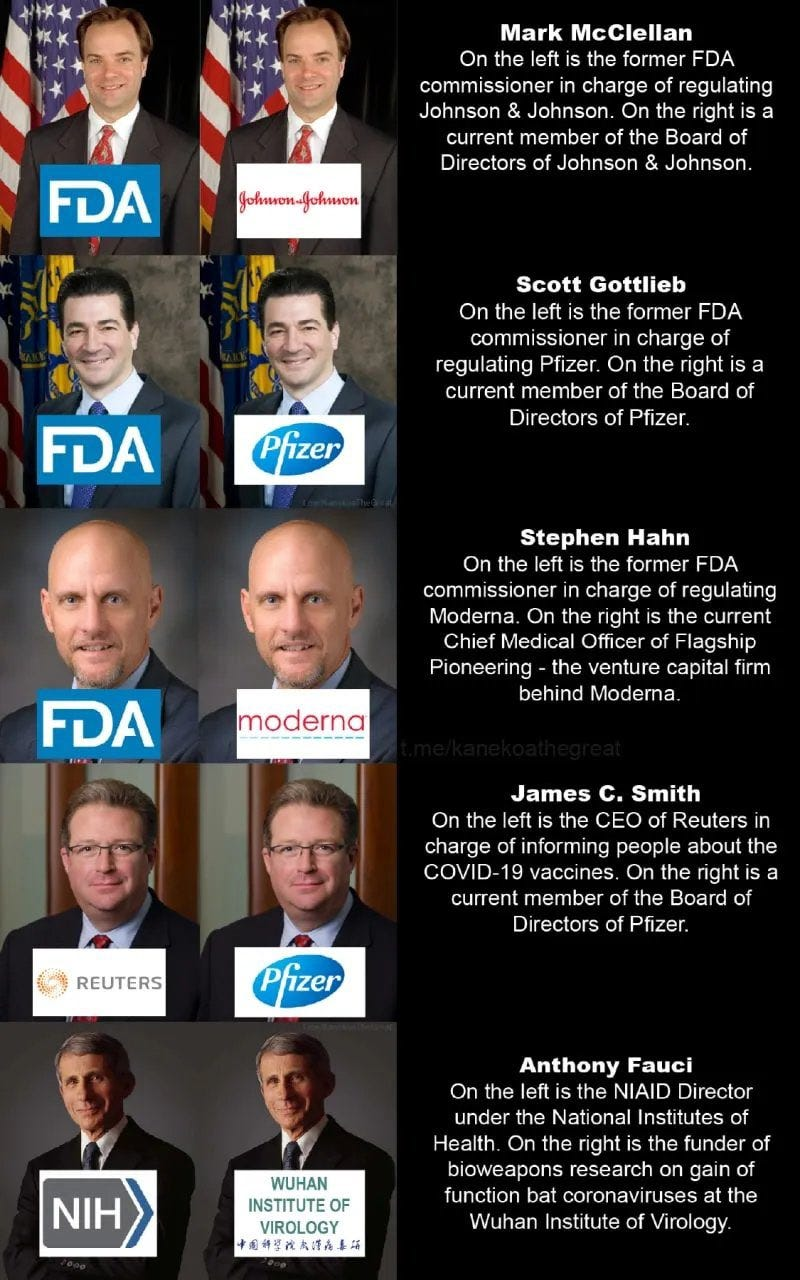
Brazen Conflict of Interest - USA Health Authorities — Click to enlarge
You may reasonably ask, "How did this occur?". Here in Australia there has been a network of high-ranking people in Government and the State & Federal Public Service who have had a long history of involvement with, and significant financial interests in, the vaccine industry. You can read about them here. In the USA there is also a very serious problem as shown by the graphic to the right, revealing the compromised and potentially corrupt state of health regulation in that country. The US Health Authorities are a key influencer as to how Australia's Therapeutic Goods Administration will act and regulate. Many times during the COVID emergency, it is apparent the TGA simply took advice from the US FDA and CDC without checking its veracity. The reason the personalities in the Australian Health Departments at Federal, State and Territory level reacted so atrociously as they did, may have not only been their general incompetence but also because of their own intimate involvement in the vaccine and commercial pharmaceutical industry. As for the politicians involved in this, a number of them appear to have been compromised and, almost without exception, if they possessed any talent or competence at all, it was not in the area of managing a contrived health crisis.
RNA Viruses and COVID-19. COVID-19 belongs to a group of pathogens referred to as Ribonucleic Acid (RNA) viruses. The human body is made up of cells which consist broadly of a nucleus and surrounding material called the cytoplasm. Within the nucleus there is DNA which splits to produce RNA that then exudes from the nucleus into the cytoplasm where components within the cytoplasm convert that RNA into proteins necessary for the development and wellbeing of the body. The cytoplasm is encapsulated by a cell wall. RNA viruses infiltrate the cell wall through external compatible receptors and, through complex organic chemical reactions, use the cell's components and genetic material to create components of the particular RNA virus which then reassemble within the cell's cytoplasm. These replicates then exit the cell and go on to perform the same process in other cells until they have overwhelmed their host.
The Importance of Vitamin D. There is a strong, established correlation between low Vitamin D and one's susceptibility to and, if infected, the severity of, diseases caused by RNA viruses. (For a far more detailed explanation of this, please click here to watch a video featuring Dr Sebastian Rushbrook and Dr David Grimes; someone who has studied this matter in great detail over many years. It is a fascinating interview.) This correlation is sufficiently strong enough to suggest that low Vitamin D is linked to causation. Vitamin D is not actually a vitamin. It is more like a hormone and it is created in the liver and kidneys from a precursor that is created in the skin when it is exposed to sunlight or UV-B rays. (Ultraviolet B (UV-B) is electromagnetic radiation, usually from the sun, with wavelengths between 290 and 320 nm. It comprises less than 1 per cent of the ultraviolet radiation that reaches the earth's surface.) The human body then converts the vitamin D precursor into a hormone often referred to as activated vitamin D or calcitriol. Because this process needs sunlight containing UV-B, dark skinned people and all people living in cold climates are likely to suffer from Vitamin D deficiency. (UV-B does not pass through window glass, but will pass through clear quartz.) The ability of the body to create activated Vitamin D drops off significantly after 50 years of age. Wearing sunscreen blocks UV-B and so reduces Vitamin D production but the disadvantages of this have to be weighed off against the dangers of skin damage and cancer that can be caused by excessive exposure to UV-B. Vitamin D plays a vital role in helping the human body have healthy mucosa, good bones and general good health. The typical level of Vitamin D in the blood should be around 25 ng/ml (for nanomoles per litre, multiply this figure by approximately 2.5). An inexpensive blood test can accurately check this and if it is low a supplement can be taken on a daily basis to correct this. Typically, 2,000 International Units taken in the morning and in the evening will raise the Vitamin D level in a healthy adult to around 35ng/ml. If in doubt, a GP should be consulted. Please note that large injections of Vitamin D have been shown to be of little use. Vitamin D, like fertiliser is for plants, needs to be present in the body at normal or moderately higher levels for quite a period of time before the full benefits of Vitamin D will be acquired. Taking Vitamin D once ill with COVID is not as effective as taking it on a continuous basis in moderate amounts per your doctor's recommendations.
The Importance of Zinc. There is also a strong correlation between low Zinc levels and severity of disease with respect to RNA viruses. A high level of Zinc in human cells will, in most cases, interfere with RNA dependent RNA polymerase (RdRp) which is used by RNA viruses to replicate within human cells. (Click here to learn more) Zinc cannot easily find its way into human cells and is generally carried there attached to other chemical complexes which have the ability to pass through the membranes of human cells. These compounds are called "Ionophores". So if you should be feeling a cold or sore throat coming on, you simply need to take Quercetin (an ionophore - more on this below - available at Chemists and Health Food Stores without prescription), Zinc & Vitamin C (one such product is "Zinc Advanced" made by FUSION Health - but there are many other manufacturers also) and Aspirin (typically 100mg daily unless you are already taking an anticoagulant). If taking Quercetin, Vitamin C, Zinc and Aspirin, as well as drinking lots of fluids, does not appear to be improving the situation within a period of 12 hours from first commencing treatment, seek urgent medical attention. It may be that you are dealing with a bacterial rather than viral infection. Bacterial infections such as Streptococcus pneumonia and Meningococcal disease can be swift and deadly. Because of mask mandates, infection from Streptococcus Pneumoniae, in particular, has become more prevalent. (Masks are not only useless, they are positively dangerous in many different ways! I will deal with that in greater detail later in this webpage.) As a general rule, anyone who presents with serious chest congestion and apparent infection should have a sputum sample examined by pathology to determine if they have a bacterial infection and the antibiotic most appropriate for its treatment. My reading of medical literature suggests that Doxycycline, Azithromycin or Bactrim are all likely to be good for situations such as this but analysis of the sputum by pathology is by far the best approach to ascertaining the ideal treatment.
The Role of Quercetin. Quercetin belongs to a class of organic compounds called "lysosomotropic ionophores". This long name simply means that Quercetin has the ability to enter human cells and that it attracts the Zinc cation (Zn++). In doing this, Quercetin transports the Zinc into the cytoplasm of the human cell where it effectively interferes with RNA viral replication. Vitamin C acts as a "helper" in this process. With rest, drinking lots of water and taking this medication, most people will be a lot better within 2 days of starting to feel the onset of a cold, rhinovirus or flu. As they say, "Should symptoms persist or get worse, see your doctor as soon as possible" but within 2 days you should be noticeably better. You should continue this treatment for another 3 to 5 days just to be sure there is no rebound.
Hydroxychloroquine (HCQ) and Ivermectin (IVM). HCQ and IVM are also, like Quercetin, ionophores which can pass through the membranes of human cells but they also have other curative attributes. HCQ is known to reduce inflammation and moderate immune response. That is why it is used for the treatment of Lupus and Rheumatoid Arthritis. IVM upsets viral activity by a number of mechanisms. To learn more please click on this short paper which deals with that subject.
Unfortunately, both Ivermectin and Hydroxychloroquine require that you obtain a prescription and, here in Australia, the Australian TGA and Health Authorities have inexplicably banned doctors from prescribing it to treat COVID-19. That is why I suggest Quercetin which does not require a prescription. It is most probably not as powerful as HCQ and IVM but, in most cases, it is, according to Prof Dr Peter McCullough (someone I greatly admire) quite effective.

Dr Raoult - Effect of Combining Azithromycin with Hydroxychloroquine
The Need to Combine Various Medications to gain Maximum Effectiveness. One of the few good things that have come out of this dreadful chapter in modern human history, is the emergence of some truly exceptional people such as Prof Dr Didier Raoult, Dr Vladimir Zelenko, Professor Dr Peter McCullough, Dr Tess Laurie, Prof Dr Dolores Cahill, Prof Dr Thomas Borody.... and the list goes on. Prof Raoult first came to my attention when he published a graph showing the results he was achieving by using Hydroxychloroquine in combination with Azithromycin.
Fluvoxamine. Another exceptional person who, interestingly, like me is not a doctor of medicine, is Mr Steven Kirsch, an electrical engineer, entrepreneur, inventor and very successful businessman. He has been very active in researching the value of Fluvoxamine for the treatment of COVID and "Long-COVID". Steve is an exceptional person on many levels but his research into the value of Fluvoxamine has been outstanding and, I believe, significant. Fluvoxamine is a close relative of Prozac and it has the ability to cross the blood brain barrier. Besides being one of a number of low cost therapeutical medications that appear to be most effective in the early treatment of COVID-19, Fluvoxamine distinguishes itself in that it not only appears to be most effective for the treatment of COVID-19 but also, most importantly, for the treatment of "Long COVID". Related to this, Fluvoxamine may be beneficial for treating brain fog and confusion, caused by the S Protein, generated by mRNA injections, which finds its way into brain cells and the brain's micro-vascular system. To learn more about the benefits of Fluvoxamine, please click here; "The Case for Fluvoxamine in the Treatment of COVID-19 and Long COVID."

Case Fatality Rates - without & with Early Treatment (click to enlarge)
Data source - US CDC
1. Case & Infection Fatality Rates (CFR & IFR) of COVID-19, with early treatment, may be less than Influenza - particularly for young people
For young, medically fit persons below the age of 30, COVID-19 is estimated to be around 5 times less dangerous than common Influenza. To learn more from one of the world's leading experts, Dr John P.A. Ioannidis, (Professor of Medicine and Professor of Epidemiology and Population Health) click here. Note that this publication dates back to 20 May 2020 at a time when effective therapeutics were not in wide use and were not being widely publicised. Dr Ioannidis's major expressed concern has always been about the paucity and poor quality of the data upon which incredibly important decisions are being made. His paper therefore deals with the IFR when no effective, early treatment is administered and when data was not comprehensive. Also note that the Infection Fatality Rate is far less (possibly up to 5 times less) than the Case Fatality Rate. The former counts all instances of infection whereas the latter only counts those persons who are so sick as to become "Cases". The infection fatality rate of COVID-19 under the present treatment regimen, which, in Australia, is to leave sufferers to get over this disease without effective medication until they need hospitalisation, is, across all age groups, approximately the same as a bad influenza season. I have said, "under the present treatment regimen" deliberately because here, in Australia, inexpensive therapeutic drugs which have now been conclusively proven to be highly effective in the early treatment of COVID-19 are being denied to the Australian people by the Therapeutic Goods Administration of Australia.
For more details regarding this scandalous situation please watch the following video featuring Craig Kelly (MP) and Dr Vladimir Zelenko (a person for whom I have the greatest admiration).

Australian Government - Age of Death - COVID-19 (click to enlarge)
2. Average Age of Death of Sufferers of COVID-19
The Australian Government Website, provides a graph of the age and gender of the people dying from COVID-19 in Australia. It is 86+ years of age for females and 82+ years of age for males. Very few young people are dying from this disease and those that are have other life-threatening medical conditions. In addition to this, none of those that have died received any effective therapeutic drugs during the 1st week of their infection.
A study conducted, in 2021, by Israel, found that, all persons who suffer this disease and get well are likely to have life-long immunity significantly superior to that which is conferred by any of the present vaccines. Most young people don't even realise they have had the disease. As stated above, the IFR for this disease is around 5 times less dangerous for young, medically fit persons than is the case with common influenza.

Initial Exaggeration of Deaths from COVID in Sweden (click to enlarge)
3. Initial Exaggeration of Deaths from COVID in Sweden
Initially there was an orchestrated campaign to exaggerate the danger that COVID-19 posed. This was most famously the result of a computer model developed by a Public Health Professional, Professor Neil Ferguson, in Britain who had a history of getting things badly wrong. Professor Ferguson led the COVID-19 modelling team at Imperial College in London. He resigned May 5 from his government advisory role as a consequence of scandal and the obvious fact his predictions were grossly inaccurate. Ferguson led the Imperial College team that designed the computer model that, among others, had been used to justify the stay-at-home orders in England as well as in the United States. Most sensible people have now come to the conclusion the model was so highly flawed it never should have been relied upon for policy decisions to begin with.
However this exaggeration and fear-mongering was not limited to just Britain. It seemed to permeate throughout the world as if centrally organised by the Chinese Communist Party simply, in this case, harnessing the avarice of the Pharmaceutical Industry and gigantic asset managers such as Blackrock and Vanguard who stood to make billions from instilling panic worldwide.
In the graphic opposite, is a plot of the deaths that were ascribed to COVID-19. The blue histogram shows the deaths that were initially blamed on COVID. The red plot represents the actual deaths determined through postmortem examination of the death certificates. (I personally rang the Östergötland Health Authority to verify the authenticity of this graph and its data.)
This graph reveals a 7 times exaggeration of the lethality of COVID-19.

Lima - Red vrs Other Peruvian States Taking IVM (click to enlarge)

Africa - Comparison of areas Taking IVM (click to enlarge)
4. Low Cost, Effective Therapeutic Drugs are being denied to the Australian people
Professor Dr Peter McCullough, Professor of Medicine, Baylor University, Austin Texas, Dr Brian Tyson and Dr Vladimir Zelenko (who has now been responsible for the treatment of well over 6,000 COVID-19 sufferers) estimate that hospitalisations are reduced by greater than 80% if sufferers of COVID-19 are treated at the earliest possible opportunity with Ivermectin, Doxycycline, Zinc, Melatonin and an anticoagulant appropriate for the sufferers medicinal circumstances. This being the case, if sufferers were treated as soon as symptoms present with these therapeutics, the IFR of COVID-19, including variants, would be far less than that of Influenza.
To see the effect that Ivermectin had in reducing the case fatality rate in Peru, South America please click here.
Professor Dr Thomas Borody, the creator of a highly effective composite medicine for stomach ulcers, has had a composite medication for COVID-19, based around Ivermectin, for well over a year now. If early treatment with Ivermectin, Doxycycline, Zinc Sulphate or Acetate, Aspirin or similar anticoagulant, Melatonin, Fluvoxamine... (and the list goes on) then COVID-19 has an infection fatality rate far less than that of Influenza; especially for the young and medically fit. Click here to read a paper on Ivermectin. Note that the Australia Government's Therapeutic Goods Administration is preventing the widespread use of this lifesaving composite medication. To read about this, go to the TGA Site by clicking here.
5. Masks do not in any way inhibit the spread of COVID-19

Mask Ineffectiveness - Montana vrs Wyoming (click to enlarge)

Mask Ineffectiveness - California (click to enlarge)

Mask Ineffectiveness - Memphis (click to enlarge)

Mask Ineffectiveness - New Mexico (click to enlarge)
There is no empirical data that supports the belief masks are effective in stopping the spread of COVID-19. To learn more about this click here. In fact, there is an abundance of empirical evidence which indicates masks actually increase the spread of this disease; the prime means of propagation being by contagion - hence the reason why washing hands is an effective means of reducing the spread of the disease in places like pre-schools. Masks also do physiological and psychological damage to long-term wearers; particularly teenagers and children. A recent trial was performed in Denmark which showed no appreciable difference, outside of the margin of statistical error, between wearing masks and not wearing masks. If you are still unconvinced, I suggest you click here to listen to Dr Stillwagon not only point out the dangers of wearing a mask but also the dangers that are inherent in the vaccines people are being encouraged to submit to.
How Do Masks Spread COVID-19. When people speak, tiny droplets of spit issue forth from their mouths, especially when uttering consonants. It is reasonable, therefore, to conclude that masks will stop this tiny spray of spit from infecting someone else. In their ignorance, the advocates of mask-wearing do not realise that saliva (commonly called "spit") contains a substance called salivary amylase; an enzyme - the role of which is to cleave starch as a precursor to digestion. The surface of a virus is covered in a protein and sugar. This coating is reactive and quite fragile. It has to be in perfect condition to latch onto the receptors (called ACE2 receptors) of cells comprising the epithelium of human mucosa (special tissue that issues mucus). If there is the slightest defect in its formulation it will not mate. That is why animal viruses do not normally infect humans. The protein on animal viruses is slightly different to that of viruses that infect humans and so cannot mate with human ACE2 receptors. Salivary amylase chemically attacks and degrades the surface of any virus such that the probability of it being able to latch onto human cells is very low. The mucus in an infected person's nose, however, is laden with pristine virus which means that virus-laden mucus will end up in the face mask's tissue or cloth. When that happens, the infected person will periodically touch their itchy, moist, infected facemask transferring mucus and virus to their fingers. When these persons contact commonly touched items in the public space, such as door handles, file folders, toilet doors, tap handles, etc they will transfer mucus and virus to these objects. Anyone touching those items soon after will end up with virus and mucus on their fingers. If they then pick their nose or rub their itchy eyes, they will infect themselves. That is why masks worn for long periods of time are such a bad idea. They actually help to spread the disease in public spaces. If a person is infected, they are effectively wearing a snot-laden handkerchief on the front of their face. Not a good idea. So why is Government pushing this? This is an object example of how bad the advice Government is being given and how stupid/gullible politicians (and the general public) are to believe it.
Masks do a great deal of physiological and psychological harm to those who have to wear them for prolonged periods of time; particularly children. They confer on the users no benefits at all.
6. All of the COVID-19 Vaccines carry an unacceptable risk

(click to enlarge)
All of the vaccines that are being used to vaccinate the public have not been thoroughly tested and many eminent specialists in the field of epidemiology, virology and immunology, including some who were intimately involved in the development of these vaccines, are strongly opposed to their universal use on the public. At this moment, the Vaccination Adverse Event Reactions System (VAERS) reports well over 10,000 people have died from vaccination in the US. Hundreds of thousands of people have suffered severe, disabling adverse reactions. Many claim that VAERS, being a voluntary system of reporting, understates the actual number of fatalities. (I have personally downloaded the data from VAERS and put it into a relational database. I can personally attest to the veracity of claims that thousands of people in the US have died as a result of vaccination. Click here to see the VAERS Report as at 20Sep21. It doesn't make for good reading.)
To fully grasp the seriousness of the present situation which is going largely unreported, I urge everyone to read this report by David John Sorensen & Dr Vladimir Zelenko.
Setup for a mass extinction? Adding to this concern is a published research on the development of a corona virus vaccine. This research showed that it was possible to vaccinate animals with a corona virus vaccine and then later expose them to a tailored corona virus which would kill all of them by way of pulmonary immunopathology. ("Immunization with SARS coronavirus vaccines leads to pulmonary immunopathology on challenge with the SARS virus") This is real. It is not imagined. So one has to ask why has there been such a strong drive to vaccinate people against a disease, which if early treatment using cheap effective medications was permitted, is less dangerous than common influenza? Something just doesn't compute.
If you want to obtain data from the US VAERS System, click here.
Australia also has a system of adverse event reporting. As at 7 Sep 2021, this report lists all of the adverse events of which there are 46,438 with 448 deaths deemed as likely being due to the vaccines.
7. COVID-19 Vaccines do not stop infection and do not stop infected vaccinated persons infecting others

Relationship of Doses to COVID Cases (click to enlarge)

Case Rates Israel - Vaccination not effective (click to enlarge)

Percentage Of Hospitalised Vaccinated (click to enlarge)

Death Rates UK - Vaccinated worse than Unvaccinated (click to enlarge)
Cleveland Ohio Medical Clinic - Trial results. The Cleveland Ohio Medical Clinic gathered data on over 50,000 patients, relating their susceptibility to COVID and the number of COVID-19 mRNA injections they had received. In this there was a clear relationship. The more injections, the greater the risk of infection, hospitalisation and death.
Israel. Israel is one of the most heavily vaccinated countries in the world. From the table opposite it can be seen that the majority of people in hospital are vaccinated persons. This suggests the vaccines are not effective against variants.
Added to that, a large-scale study out of Israel, conducted on over half a million people, compared the immunity of patients who had received two doses of the Pfizer/BioNTech injection to unvaccinated people who had been previously infected. Alarmingly, the study also found that people who had been vaccinated have a 13-fold increased risk of breakthrough infection from the dreaded Delta variant, compared to the previously infected.
Some propaganda outlets, masquerading as "fact-checkers", have asserted that vaccination is far safer than contracting COVID-19 and recovering from it. For young people this is not true. The number of deaths and serious injuries from COVID-19 vaccines far outnumbers the number of young people who have died so far from COVID-19 and its variants. The risk of death or serious injury from this disease is further reduced if known effective therapeutics, such as Prof Borody's composite medication, are used as soon as symptoms present.
8. Antibody Dependent Enhancement (ADE) and Other Issues
A number of specialists in the field have warned that persons who have been vaccinated could experience a phenomenon called Antibody Dependent Enhancement (ADE) when they are exposed to variants of the pathogen for which they have been vaccinated. In a significant number of instances this will be fatal. It is noteworthy that Israel, one of the most vaccinated countries in the world, is presently facing a huge rise in cases and that a significant percentage of those that are dying had been fully vaccinated. Professor Peter McCullough is suspicious that some vaccinated persons are not only experiencing a form of ADE but also the prime cause of variants that are now infecting the vaccinated as well as the unvaccinated.
This view is also shared by Professor Dr Geert Van Den Bossche.
Mass vaccination of the population is not the correct solution to this particular medical crisis. (Click here to listen to a discussion between Dr Robert Malone and Dr Geert Van Den Bossche on this subject.)
Professor Dr Dolores Cahill has extensively researched the science of mRNA vaccines and has trialled this technology on animals. All of these trials ended badly for the animals involved. She is gravely concerned that there is a strong possibility of these vaccines causing a great deal of harm to a large segment of the vaccinated population. That may already be happening in Israel. Note that Palestine has very low vaccination rates and a correspondingly low number of cases.
In this video Dr. Richard M. Flemming independently confirms much of what Professor Cahill asserted in early 2020. For this her tenure at Dublin University was terminated. Dr Fleming and Prof Cahill both contend that COVID-19 and the mRNA vaccines are both bio-weapons being employed against a malleable population of law-abiding, trusting citizens.
I strongly suggest you watch this video in its entirety. It features Dr Vladimir Zelenko. I had the pleasure of sitting in on a Zoom meeting with Vladimir last year. I was extremely impressed by his knowledge, eloquence, sincerity and his intelligence.
9. It's Happening - The Carnage caused by mRNA Vaccines
The following graphs provide some indication of the carnage being wrought by these vaccines.

Graph 1: Athletes Collapsing and Dying (click to enlarge)

Graph 2: Australian Excess All-cause Mortality, Dr Wilson Sy (click to enlarge)

Graph 3: Deaths & Serious Injuries - US Dept of Defence Medical Database (click to enlarge)

Graph 4: All-cause Mortality USA 25-44 years of Age (click to enlarge)

Graph 5: Relationship between Rate of Injections and Excess Deaths in Australia (click to enlarge)
Graph 1 relates to the increase in deaths amongst athletes from sudden cardiac incidents: the only logical cause for this being that sport authorities stupidly mandated that all athletes had to submit to Anti-COVID Injections even though this group was one of the least likely to be endangered by COVID-19.
Graph 2 shows Australian excess all-cause mortality from 25 July 2021 to 2 July 2023, compiled by Dr Wilson Sy.
Graph 3 shows the sudden uptick of deaths and injuries occurring in the US Military as reported by the Dept of Defence Medical Database. This database has been subsequently shut down with the DoD claiming there is a fault in the system such that the figures are exaggerated.
Graph 4 shows the increase in all-cause mortality rates since vaccination began. Not shown here is the difference between vaccinated and non-vaccinated persons. It is reported that insurance companies are reporting an increase in deaths above the average by 40%. See this video to gain a full picture as to the nature of these excess deaths.
Graph 5 shows the relationship between the rate of Anti-COVID-19 Injections and the rate of deaths. Many of the deaths occur within 3 days of the injection.
10. What should be the approach to COVID-19
The Australian Federal Government needs to make an unequivocal stand on this matter and follow Sweden's example. Namely:
- There should be no closure of State borders,
- no mandatory mask wearing,
- no lockdowns,
- schools and universities should continue business as usual, and
- there should be no compulsion by Government and/or private/business organisations for people to be vaccinated. This includes forbidding any type of vaccine passport or discrimination against the unvaccinated.
In addition to Sweden's example, I recommend the Australian Federal, State and Territory Governments do the following:
- ensure that the recording of death from COVID is rigorously accurate, ie, that people dying with COVID are not recorded as having died directly as a result of COVID,
- give all General Practitioners (GPs) maximum freedom to treat their patients as best they see fit but have in place a system such that the experience of all doctors and their patients can be easily (ie, without onerous clerical effort) shared for the common good,
- recommend to everyone that they have their Vitamin D and Zinc levels checked and where either of these are below normal, consult with their GPs as to how this deficiency might be corrected,
- recommend to the public that they take a daily supplement of Vitamin D, and
- recommend to everyone that, should they experience the onset of cold or flu-like symptoms they immediately take Quercetin, Zinc and Aspirin and, if the situation does not improve within 24 hours, see their GP as soon as possible.
With respect to the use of this novel mRNA technology, the following should have been and should be implemented as soon as possible:
- These injections are suspected of harming the vascular and the immune system and, for that reason, any person who is about to be subjected to these injections should have their health state established by the relevant tests before undergoing a course of injections. After each injection, the health state of the person should be similarly reviewed to determine if there has been a change that might be concerning. Their health state should be routinely reviewed at a periodicity, agreed by the medical profession, after the course of injections for at least a year.
- All persons who die within one year of the injections of a prescribed cause of death, such as, for example, cardiac failure, stroke or sudden onset of cancer, should be subjected to an autopsy that should routinely include a histological examination of their organs and relevant tissue to determine if the injections may have contributed to their death.
- The government should develop a mobile phone and desktop application that allows persons who have been injected to report their experience directly to the Database of Adverse Events Notifications. All persons who have been injected should be required to do this in order to receive their Medicare benefit provided for the purpose of the injections. This report should automatically be forwarded to their nominated General Practitioner. This would ensure a more comprehensive reporting of Adverse Events than is presently the case.
In October, I crafted a letter which was sent by registered mail to the Prime Minister of Australia, the Deputy Prime Minister, Premiers of States and Chief Ministers of the Territories. Information addressees were the Health Ministers, Chief Medical Officers and Commissioners of Police, Federal, State and Territory. This letter was signed by Prof Dr Peter McCullough, Prof Dr Dolores Cahill, Dr Tess Lawrie and Dr Robert Brennan.
You can click here to read that letter.
To download the PDF version of this letter please click here.
Its purpose was to fully inform those in power of the facts in the hope they would change their present course and adopt the recommendations shown above. As at the time of writing this has not been the case.
After waiting 6 weeks, and not having received a reply from any of the 33 addressees, I wrote a letter to the Directors of Public Prosecution at Federal, State and Territory level.
You can click here to read that letter.
To download the PDF version of this letter please click here.
11. Use of Known Effective Therapeutical Medicines
This crisis could be over in a week if the TGA authorised the use of the late Professor Thomas Borody's highly effective composite medication, based around Ivermectin, for the early treatment of COVID-19 and its variants. The widespread use of this medication would reduce the IFR of COVID-19 to a level significantly lower than that for influenza. Further reinforcing this, if Health Authorities encouraged all vulnerable persons to have their Vitamin D and Zinc levels checked and for GPs to remedy any that are below normal, the incidence of this disease would be significantly reduced as would its severity.
For a more detailed treatise on this subject please click here.
Here is a list of very interesting videos and presentations made by Prof Dr Peter McCullough, someone I count as a friend and whom I greatly admire for his integrity, courage and intellect:
- "Dr Peter McCullough lecture on the State of COVID Treatment", recorded at the Andrews University Village Church, Berrien Springs, MI, August 20, 2021
- "How to Treat Long Haul Covid-19", presented October 2, 2021 at the AAPS 78th Annual Meeting Held in Pittsburgh, PA.
(My sincere thanks to Tracy Bergquist for her editing of this page and her suggestions on how it might be improved.)
- End of Paper -